Root Canal Treatment in Edgware
Modern root canal treatment to save an infected or damaged tooth — gentler than its reputation, and far better than losing the tooth.
Book Online opens in our secure Dentally Portal — verified by SMS. All treatment plans start with a check-up.
from £350
- Saves your natural tooth
- Removes pain caused by infection
- Stops infection spreading to surrounding tissue
- Single visit possible for many front teeth
- Modern techniques are far gentler than the procedure's reputation
When is root canal treatment needed?
Inside every tooth is a soft tissue called the pulp, which contains nerves and blood vessels. When the pulp becomes inflamed or infected — through deep decay, repeated treatment, a crack or trauma — you may feel:
- Persistent toothache, especially with hot or cold food and drink
- A throbbing pain that wakes you at night
- Tenderness or swelling in the gum around the tooth
- A bad taste or visible discharge
Without treatment, the infection can spread to surrounding bone and tissue and ultimately into the wider face and neck. Root canal treatment removes the infected pulp, disinfects the inside of the tooth, and seals it — saving the tooth and resolving the pain. For most patients it’s a far better outcome than losing the tooth and dealing with the consequences of a gap.
At Campos Dental we treat root canal cases for patients across Edgware, Stanmore, Mill Hill and the surrounding North London area. The page below explains how the procedure has changed over the last twenty years, why much of the procedure’s bad reputation no longer reflects reality, and what to expect when you come in.
Why root canals have a bad reputation — and why that’s outdated
If you ask any group of adults what they think of root canal treatment, you’ll hear the same words back: painful, dreaded, last resort, something to avoid at all costs. The reputation is deeply held, and it has very little to do with what the procedure actually involves today.
Most of the bad reputation dates to root canal treatment as it was done in the 1970s and 1980s. Diagnosis was less precise, anaesthetic technique was less refined, files were used by hand for long stretches, isolation of the tooth was less reliable, and follow-up imaging was limited to two-dimensional X-rays that often missed the detail. A root canal performed under those conditions could indeed be a long, uncomfortable, hit-and-miss procedure.
Modern root canal treatment — performed today, with the techniques and equipment that have become standard across UK private dentistry — is a very different experience. The procedure is performed under reliable local anaesthetic and most patients describe it as feeling much like having a large filling. The pain people came in with is typically gone by the time they leave. Patients tend to be surprised at how undramatic the appointment turns out to be compared with what they had braced themselves for.
The honest framing — root canal isn’t an experience anyone goes seeking, but the modern version of it is one of dentistry’s most reliable ways to save a tooth that would otherwise be lost. The genuinely difficult part is the toothache that brings you in, not the treatment that resolves it.
Modern endodontic techniques
A few specific improvements have made the difference between modern root canal treatment and the version your parents remember. We use the following as standard at our Edgware practice — none of these are exotic equipment, all of them are commonly used in modern UK private dentistry.
Rotary nickel-titanium instruments
The files used to clean and shape the inside of the canals are now driven by a slow electric handpiece and made from a flexible nickel-titanium alloy. The older hand files were stiffer steel, used manually for long sequences, and tended to be slower and less precise. Rotary instruments shape the canal more accurately in a fraction of the time and follow the natural curve of the root rather than fighting it. This is the single biggest reason the appointment is shorter and more comfortable than the procedure used to be.
Rubber dam isolation
A thin sheet of latex (or latex-free alternative for allergy-prone patients) is placed over the tooth being treated, isolating it from the rest of the mouth. The rubber dam keeps saliva — which carries bacteria — away from the canals during treatment, keeps disinfecting solutions on the tooth and off the soft tissues, and stops anything dropping into the back of your throat. It looks slightly unusual when you first see it but it’s quickly forgotten, and the difference it makes to the predictability of treatment is significant. Modern endodontic protocols essentially require rubber dam — a root canal performed without one is working at a disadvantage from the start.
Magnification
Working at significant magnification — through dental loupes or a clinical microscope — lets us see canal anatomy in much more detail than the naked eye allows. The internal anatomy of teeth is more variable than it looks on textbook diagrams; some molars have an extra canal that’s narrow and easily missed without good magnification. Better visualisation means more reliable cleaning and a lower chance of leaving disease behind.
3D imaging where indicated
For complex cases — re-treatments, suspected fractures, unusual anatomy on the standard X-ray — a small cone-beam CT scan gives a three-dimensional view of the tooth and surrounding bone that ordinary 2D imaging can’t. We don’t take a CBCT for every case (most cases don’t need one), but having the option avoids the older situation of “open up and hope.”
None of this is presented as marketing — these are the standard tools modern endodontic protocols rely on. The improvement they deliver collectively is the reason published success rates for root canal treatment now sit in the 86–95% range at ten years.
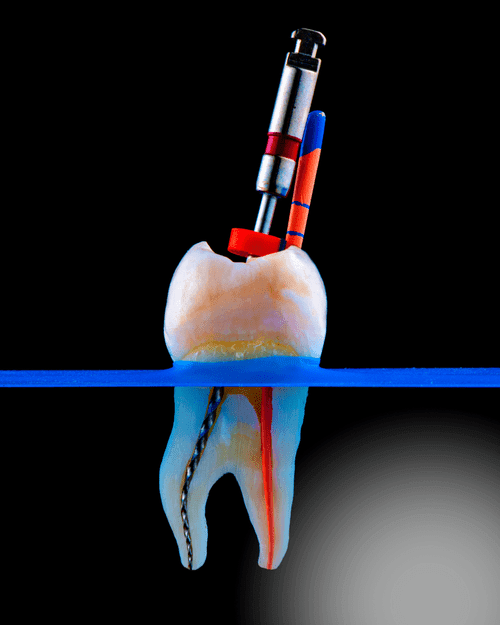
Accessing the root
To treat an infected pulp, your dentist needs to reach the chamber inside the tooth. A small, carefully-controlled access opening is created through the top of the tooth — just wide enough to clean each canal — without weakening the surrounding tooth structure.
The root canal procedure at Campos Dental
- Diagnosis. A clinical exam, digital X-rays, and (where needed) a 3D CBCT scan to confirm the diagnosis and plan treatment. We test the tooth to be sure the pulp is genuinely the source of pain — a small number of “tooth pain” complaints turn out to be something else (a cracked filling, a sinus issue, referred pain from elsewhere), and root canal treatment on the wrong tooth helps no one.
- Anaesthetic and isolation. The tooth is numbed completely with local anaesthetic and isolated with a rubber dam so it stays clean and dry throughout. We check the numbness is complete before any drilling begins — if there’s any residual sensation we add more anaesthetic. You should feel pressure and movement during the appointment but no sharp pain.
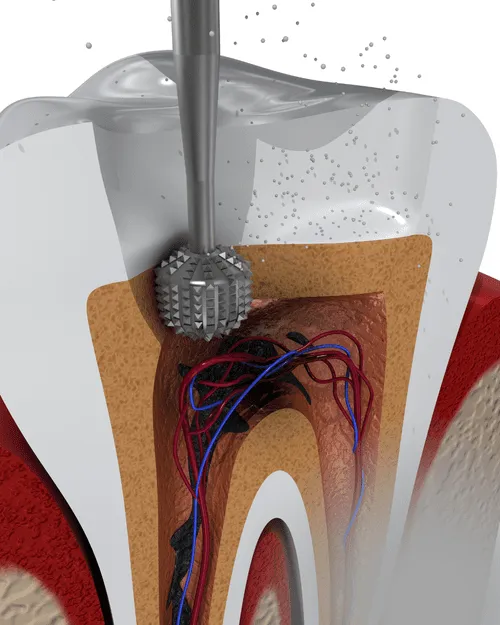
- Access opening. A small opening is made through the top of the tooth so we can reach the pulp chamber and the canals inside. We use the magnification described above to find every canal at this stage.
- Cleaning the canals. We carefully remove the infected pulp tissue using rotary nickel-titanium instruments, irrigate each canal with antibacterial solutions to dissolve any remaining tissue and disinfect the surfaces, and shape the canals ready to be sealed. For a multi-canal back tooth this is the longest part of the appointment.
- Sealing the tooth. The canals are filled with a rubber-like material called gutta-percha, sealing them against re-infection. For a tooth that’s draining or significantly infected we may dress it with antibacterial paste between appointments and seal it permanently at a second visit a week or two later.
- Restoration. A filling or crown restores the tooth’s strength and appearance. Most back teeth benefit from a crown — see the crown FAQ above.
Why save the tooth?
Modern dentistry can replace a missing tooth beautifully — but nothing quite performs like a healthy natural tooth root. Saving a tooth via root canal preserves your bite, keeps your jawbone stimulated by normal chewing forces, and avoids the more involved restoration that would follow extraction and replacement with a bridge or an implant.
The cost case is also worth understanding honestly. A root canal followed by a crown at our Edgware practice typically totals £900–£1,200 — broadly comparable to a single implant and crown, which usually runs to £2,500–£3,500. For a tooth that has a reasonable chance of long-term survival with endodontic treatment, the root canal route is almost always the better-value first option. If the root canal fails years later, an extraction-and-implant pathway remains available. The reverse isn’t true: once a tooth has been extracted, the root canal option is gone.
We’ll only recommend root canal treatment if we believe the tooth is realistically saveable. For badly broken-down or significantly cracked teeth we’ll be honest at the start that extraction is the more reliable answer — see our extractions page — and we won’t take you through a long and expensive endodontic appointment on a tooth that probably won’t last.
In pain right now?
Don’t put it off. Call us on 020 3971 2000 — we keep emergency appointments available every day and will do everything we can to see you the same day. Pain that wakes you at night, throbbing that builds over hours rather than minutes, swelling of the gum or face, or a bad taste from a specific tooth all suggest infection that needs prompt attention rather than waiting. Earlier treatment is almost always easier, quicker and cheaper than delayed treatment. If you’re not sure whether what you’re feeling counts as an emergency, get in touch and we’ll triage it on the phone.
Frequently asked
Will a root canal hurt?
How long does the treatment take?
Will I need a crown afterwards?
How much does a root canal cost?
What if my tooth still hurts after the root canal?
How long does a root-treated tooth last?
You might also be looking at.

Dental Crowns
from £550Custom-made caps that restore broken, cracked or root-treated teeth. Available in porcelain, ceramic and metal options to suit appearance, position and budget.
Learn more
General Dentistry
from £50Routine, preventative and family dentistry — the foundation of a healthy smile. Check-ups, hygiene visits, tooth-coloured fillings, and oral cancer screening for every age.
Learn more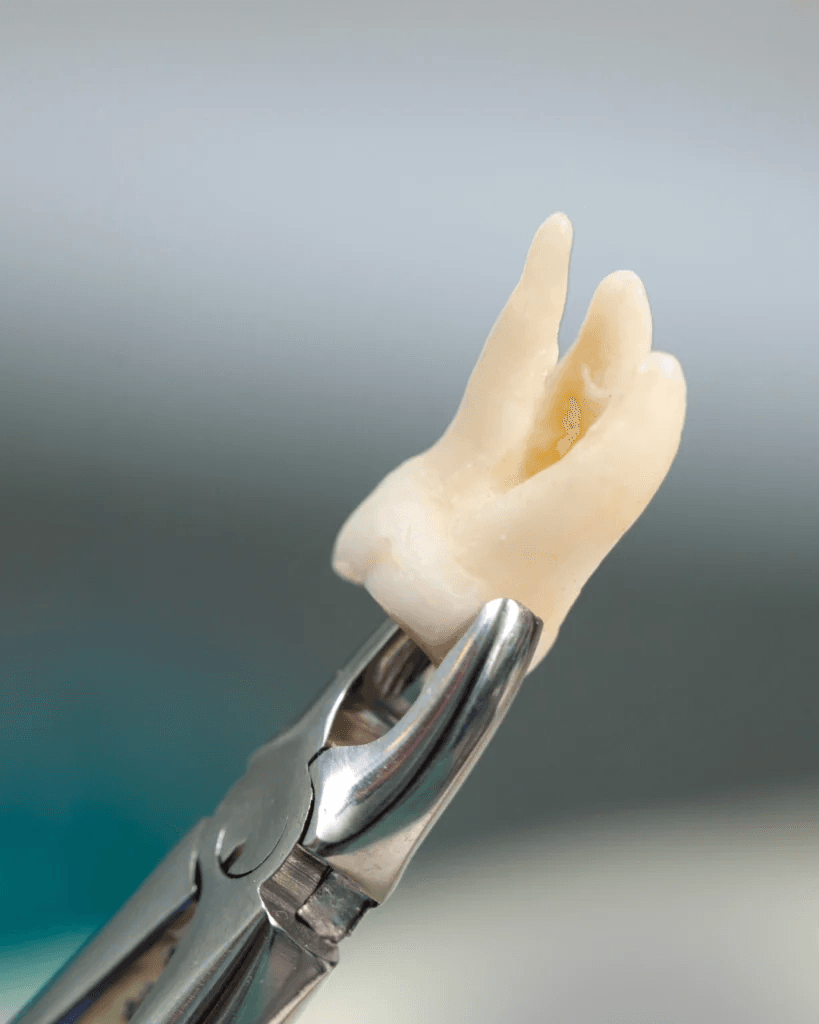
Surgery & Extractions
from £150Gentle tooth removal and oral surgery — including wisdom teeth. Performed in a calm, modern environment with sedation available for nervous patients.
Learn moreFind us in Edgware.
Free 30-minute parking out front and a step-free entrance. Pop in for a look or call ahead — we usually answer within a few rings.
Campos Dental
70 Edgware Way
Edgware, HA8 8JS
Call us
020 3971 2000Contact us
Send us a message →Opening hours
- Mon – Fri 9:00 am – 5:30 pm (closed 1–2 pm)
- Sat by appointment
- Sun closed
Considering this treatment?
All treatment plans start with a check-up. Book yours online — we'll talk you through the options for this treatment, explain pricing, and only recommend treatment if it's genuinely right for you.
Book Online opens in our secure Dentally Portal — verified by SMS. All treatment plans start with a check-up.